MM Curator summary
The article below has been highlighted and summarized by our research team. It is provided here for member convenience as part of our Curator service.
[MM Curator Summary]: Home health workers say they are not seeing the money appropriated to up their wages; MCOs say not everybody was supposed to get a raise per the legislation; the legislator who sponsored the bill that funded the increase said it was written poorly; home health agencies cry Big Bad MCOs; and Big Union blames everybody.
Clipped from: https://www.newsday.com/business/home-health-aide-medicaid-minimum-wage-mkef5db1
Home care worker Mildred Garcia-Gallery, right, assists Christine Cipriani at Cipriani’s home in Garden City South. Credit: Newsday/J. Conrad Williams Jr.
An hourly wage increase of $2 designed to help ease the shortage of home care aides is finally in place, but industry players disagree about whether the raise can accomplish its goal without collateral damage.
At stake is home care for Long Island’s growing older population. The region has around 40,140 home care and personal care aides, and is projected to see openings increase by over 64% by 2028, according to the state Department of Labor. Agencies that employ home health aides have said they had trouble attracting workers for the demanding jobs at the previous $15 an hour minimum wage in a market where workers can often make more at Target or Walmart.
In the years prior to the state’s multi-year push to a $15 overall minimum, agency advocates said aides were regularly offered starting pay above minimum wage. But as the minimum wage increased, state-assigned Medicaid reimbursements for many home care agencies did not keep pace, leaving them struggling to keep up.
Home care agencies hailed the move to $17 an hour as a victory when lawmakers included it in the state budget this spring, allocating $7.7 billion to fund it over the next four years.
But now, with the increase in effect since Oct. 1, some agencies say they’re not being reimbursed enough to cover the higher pay. They blame the insurance companies that administer the state Medicaid funds. And they say the raise could end up having the opposite effect, forcing them to reduce workers’ hours and cut staff, or even putting their businesses at risk.
On the other side, the insurance companies charge that some agency owners, already receiving adequate reimbursements, are asking for more just to pad their profits.
A workers’ union says both things are happening. And a legislator who pushed for the higher wage blames poorly crafted language in the state budget for the mess that has threatened the goal — to address the labor shortage and make more caregivers available.
“It is critical that the funds that legislators intended to go to worker pay do exactly that,” said Kathy Febraio, president and chief executive of the New York State Association of Health Care Providers, a trade group representing around 125 home care agencies.
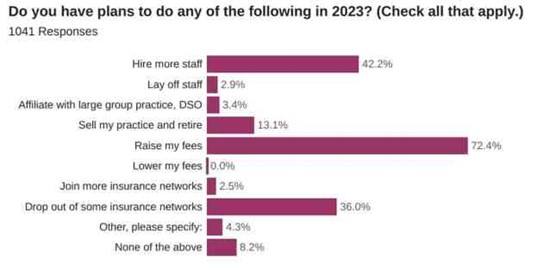
According to an Oct. 5 survey of Febraio’s membership, 75% said they were not getting reimbursement rates high enough to cover increased payroll costs. If the rates they’ve been offered weren’t raised, 29% of respondents said they would reduce staffing levels, with 72% saying they would reduce service hours.
Twelve percent of respondents said they would go out of business.
Representatives for insurance plans, though, reject the assertion that they are withholding reimbursement dollars or providing inadequate reimbursement to agencies.
Insurance plans “have been working diligently to allocate the wage funding provided to them to home care providers which in turn should be spent on workers,” said Eric Linzer, president and chief executive of the New York Health Plan Association, a trade group representing the managed long-term care insurance plans that administer the funds.
“No health plan is paying any provider less than what they need to meet wage, benefit and administrative requirements,” Linzer said. “What’s happening here is you have some providers that already have received enough funding. It kind of begs the question of why do some of them need more, other than to pad profits.”
“I’m very happy that [workers are] getting the increase,” said Nicole Laborde, who owns Ideal Home Care Services in Hauppauge, a provider of home health aides. “However, it’s going to affect a lot of home health care agencies, especially smaller ones.”
Laborde said the insurance providers aren’t providing high enough reimbursement rates to agencies.
“Nobody really looked at how the home care agencies are going to be compensated to be able to afford this increase,” said Laborde, who is also founder and chief executive of Ideal School of Allied Health Care in Hauppauge, which trains health care workers including home aides.
The wage increase is meant to help address a critical labor shortage that’s only expected to worsen as the need for home care aides grows in the coming years.
Aging Baby Boomers have increased the demand for home health services on Long Island as the preference for “aging in place” has grown, said economist Shital Patel with the Labor Department’s Hicksville office. Health care reform has also encouraged the use of home care as an alternative to expensive nursing homes and hospital stays, she said.
There are more than 1,300 licensed or certified home care agencies statewide, according to the New York State Association of Health Care Providers.
Competition for entry level workers from employers like Amazon and Target offering higher hourly wages in the wake of the pandemic has only exacerbated the difficulty in recruiting aides, who provide critical services to seniors and others living at home. Aides not only provide care, but can often become a vital source of companionship, developing close relationships with patients and their families, said aides and care recipients.
Because most patients use Medicaid to cover home care, wages for workers largely rely on reimbursement rates set by managed long-term care plans. While Medicaid is traditionally government health insurance for the most impoverished Americans, it is one of the few ways patients can cover the high cost of home care.
“There are only a few ways to pay for home care,” said Nicole Christensen, patient advocate and president of Care Answered, a Freeport business that helps families navigate the complex world of health care for seniors. Because private health insurance seldom covers home care, she said patients have three options when paying for those services: Paying out of pocket “which becomes very expensive very quickly;” long term care insurance, “which not many people have,” and community-based Medicaid, a form of Medicaid that specifically covers nursing home-level care in the home.
Agencies said they would like to see the state Health Department step in and set a standard reimbursement rate for agencies, which currently negotiate individually with insurance firms.
On average, Febraio said members of her trade organization have been receiving $1.33 per hour in extra reimbursement, half of the $2.66 the group estimated members would need to cover wage increases plus higher payroll taxes and other related costs.
“I believe the Department of Health thought the money would flow through the plans to providers and ultimately to the workers,” Febraio said. “The information that we’re giving to them is making it clear that that’s not happening.”
Linzer, representing the insurance firms, said that when the state set aside funding for reimbursement , they did not intend for every agency to receive a bump of $2 if their existing contracts had higher rates to begin with.
“The state has been very clear that this is not supposed to be a directed payment where everyone gets a $2 increase,” he said. “In instances where you have contracts that exceed the new wage requirements, there will be less of an increase.”
The median annual wage for home health and personal care aides is $31,893 on Long Island, according to state labor data, with experienced aides earning an average of $18.46 an hour.
Sen. Rachel May (D-Syracuse), sponsor of the original fair pay for home care workers legislation that failed to pass but instead was adopted in part in the governor’s budget, said the intent of increasing home care workers’ wages was to retain workers and grow the industry. Now, she said she’s concerned that if agencies aren’t given high enough rates, the wage increases run the risk of making a bad situation worse.
“The fact that the bill didn’t pass and got folded into the budget means a bunch of language we put in the bill to avoid this exact situation didn’t end up in law,” May said. “It’s the opposite of what we’re trying to accomplish here.”
The governor’s office said that due to financial measurements introduced through the Affordable Care Act, insurers handling Medicaid reimbursement cannot keep the money passed through them. Additionally, the state is encouraging home health agencies to report insufficient payments for wage increases to the Health Department.
The department will also “keep reiterating” its guidance on the matter with insurers to ensure compliance, the governor’s office said.
May said she is now working to ensure that taxpayer dollars go to adequately funding agencies so they can pay their employees more. A major structural hurdle is that the reimbursement rates negotiated between insurance companies and agencies are not disclosed to the state, making it more difficult to determine whether insurance plans are paying high enough rates, she said.
“The biggest struggle we have is transparency,” May said. “We don’t know what the terms are of a lot of the contracts.”
Mildred Garcia-Gallery, 53, a consultant, home health aide and activist, said she worked with the New York Caring Majority — a coalition of aides, agencies and elected officials —aides to campaign for higher wages in the industry and reimbursement rates to support them.
After hearing about the state’s plans to adopt a higher wage early this year, she was ecstatic. Now, she said she worries whether higher costs for agencies will mean fewer hours for workers.
“It felt like a slap in the face,” said Garcia-Gallery, who’s worked in home care for 30 years and consults with agencies through her firm Ageless Companions LLC.
She said if agencies are forced to cut hours for workers, then aides won’t be able to earn the overtime pay they need to make ends meet, resulting in picking up work with additional agencies to get by.
“I could find another job but what about these patients? If we exit, what happens?” she said. “It’s a job that I love. But loving it and surviving off of it are two separate things.”
Officials representing unionized aides said they have heard of plans paying rates too low to cover the increased costs, but also said some agencies are more concerned about profit than the wages of their workforce.
“We don’t always agree with the employers and we sometimes think they keep too much of the funding themselves,” said Helen Schaub, political director for 1199SEIU, the union representing 53,000 home care workers in the state, including 5,000 on Long Island. “You have to look agency by agency.”
Schaub said while the wage increase is good for workers, the ultimate problem is that for-profit insurance firms are involved in the Medicaid reimbursement process at all, instead of rates being negotiated directly with the state.
“What has been happening is that the state puts in money at the top and there’s this finger pointing between the employer and plans about who is keeping the money,” she said.
The $17 minimum applies to home health workers on Long Island, in Westchester and in New York City. In other parts of the state, where the minimum for most workers is $13.20, the minimum for aides has gone up to $15.20. Home care workers across the state are scheduled to receive another $1 increase next October.
Winsome Gayle Allen, 58, said the sometimes-challenging work of caring for patients at home has been a personal calling for 40 years.
“The type of work where I feel comfortable is giving my time to elderly people,” said Gayle Allen, of Hollis, Queens, an aide with Fresh Meadows-based Reliance Senior Living Services.
Gayle Allen, who’s been serving patients in New York since moving to the states from Jamaica with her parents at 19, said she’s developed long-lasting relationships with patients and their families.
While she loves what she does, she admits the work can be difficult at times and requires a lot of empathy and patience. Given the demanding hours and low wages, she said workers are in dire need of pay increases above what’s currently being offered.
“I’m not going to beat around the bush…I think we should get a starting pay of $20 an hour,” she said.
Christine Cipriani, 91, of South Garden City said she doesn’t know what she’d do if she didn’t have the support of her regular home care aide Mildred Garcia-Gallery.
“It’s vital for me,” Cipriani said. “My kids are very nice kids, but they have their own stuff to worry about.”
Cipriani said Garcia-Gallery first came into her life three years ago when the aide was looking after her husband until he died a year ago. “She’s like part of my family,” she said.
For Garcia-Gallery, helping Cipriani and other patients fills her with a sense of purpose and comes with emotional rewards.
“I like being needed and having that responsibility,” she said. “We like to do this job because we like to care for people, we love people and we love making people’s lives better or at least trying to.”
Still, she said, while the work “makes me feel important, it doesn’t mean my pay reflects that.”
For Thomas McCarthy, 24, a wheelchair user living in Farmingdale, having access to reliable home care gives him the opportunity to be more independent, he said.
“With just me and my aide helping me out, I’m not so dependent,” said McCarthy, who has Duchenne muscular dystrophy, a condition that progressively weakens muscles over time.
His aide, Marc Bazile, 52 — who lives in McCarthy’s family home every other week to provide round-the-clock care — said the work he does helping others makes him feel good and helps him appreciate the independence he has in his own life.
“I love family. I love to help people,” said Bazile, an aide with Ideal Home Care Services, who commutes from Lancaster, Pennsylvania every other week to assist McCarthy.
Still, Bazile said, pay remains an issue. As an experienced aide already making more than minimum wage, he said he hasn’t seen any impact from the recent $2-an-hour pay increase.
— with Coralie Saint-Louis